Case Studies
Case Studies
Branch Vein Occlusion
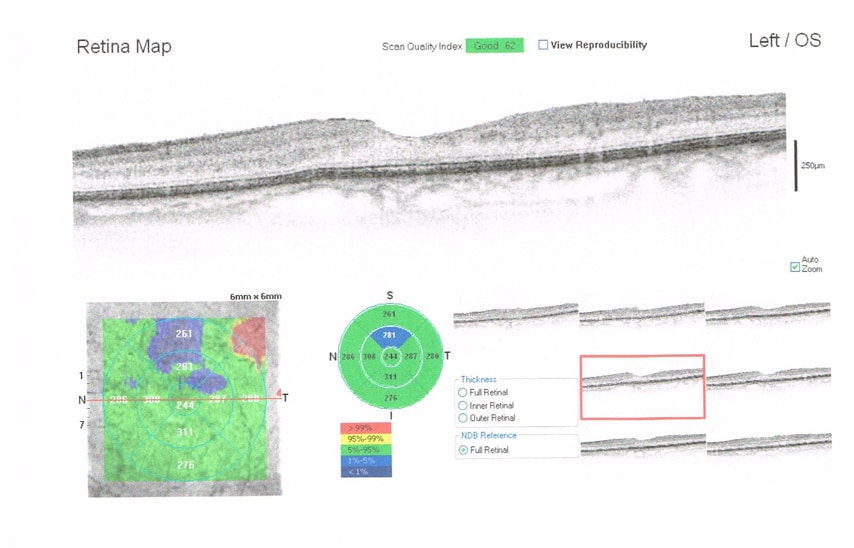
An 82 year old male presented with a history of Branch Retinal Vein Occlusion in the supero-temporal quadrant of his left eye. On examination arteriolar narrowing and arterio-venous compression was noted. The OCT image demonstrates thinning and loss of normal architecture in the supero-temporal quadrant. Mean Central Retinal Artery Pressure (MCRAP) and Ocular Perfusion Pressure (OPP) were measured using the Ophthalmodynamometry Function of the FAT1 Device.
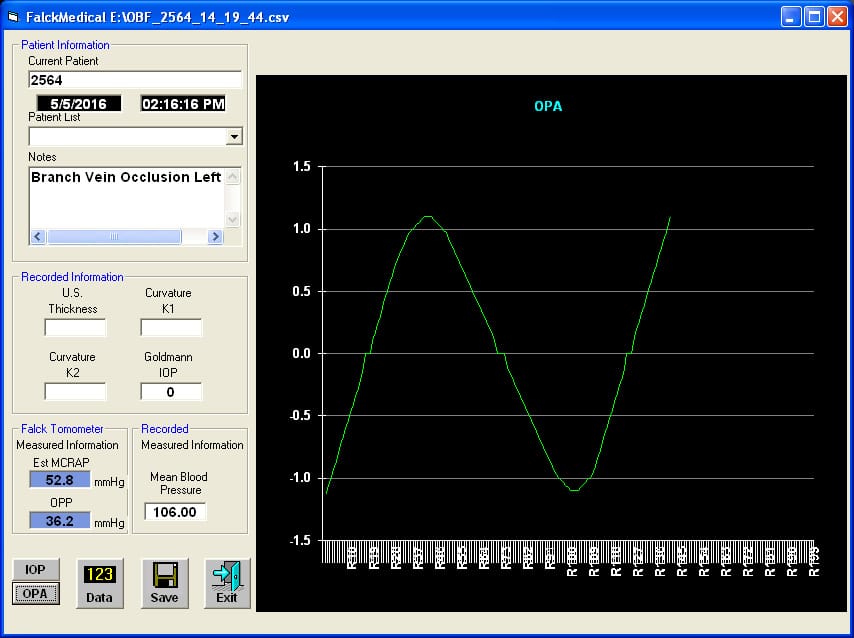
With normal vascular physiology and normal vessels, in the upright position MCRAP should be equal to or greater than 60 % of ipsi-lateral Mean Arterial Brachial Blood Pressure (MABBP). Ocular Perfusion Pressure (OPP) is the difference between MCRAP and IOP. Ocular Perfusion Pressure is the net force that drives blood flow into the eye (Adlers Physiology of the Eye, Clinical Application, Tenth Edition, Chapter 33, Ocular Circulation, page 764-765).
The measured ipsi-lateral MABBP was 106 mmHg, 60% of this value is 60.6 mmHg. The FAT1 measured MCRAP was 52.8 mmHg which is less than expected and the OPP was 36.2 mmHg which is also less than expected. See FAT1 Ophthalmodynamometry Result Screen. In the FAT1 Ophthalmodynamometry study, in healthy eyes the Average Ocular Perfusion Pressure was 44.01 mmHg. Both values are less than expected, documenting decreased retinal perfusion from the BRVO and atherosclerosis.
Amaurosis Fugax , Carotid Atherosclerosis
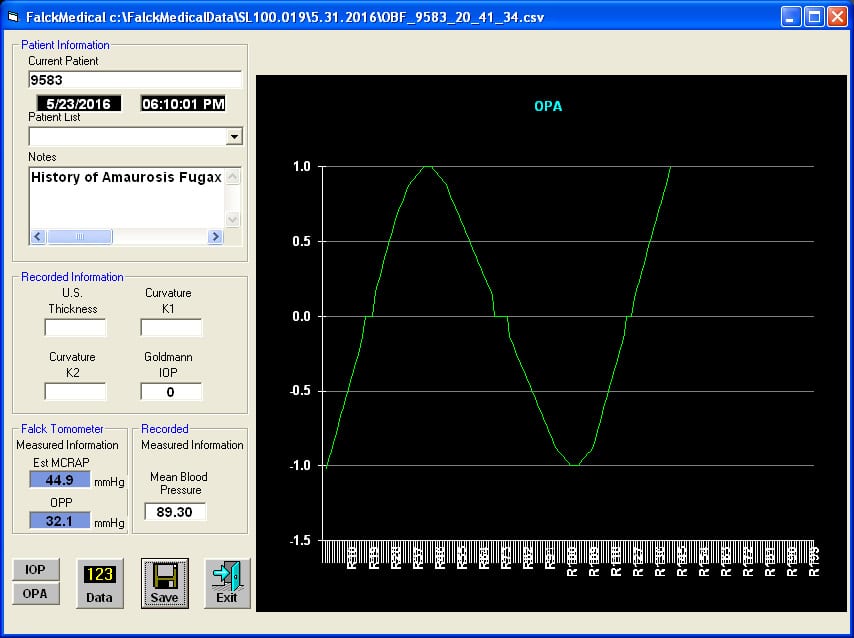
An 80 year old male presented with an episode of temporary vision loss in his right eye one week ago. No plaque or other emboli were found on examination. Using the Ophthalmodynamometry Function of the FAT1 Device, Mean Central Retinal Artery Pressure (MCRAP) and Ocular Perfusion Pressure (OPP) were measured.
Measured Mean Ipsilateral Arterial Brachial Blood Pressure (MABBP) was 89.3 mmHg. Sixty percent of this value is 53.6 mmHg. Measured Mean Central Retinal Artery Pressure (MCRAP) was less than expected at 44.9 mmHg. Ocular Perfusion Pressure (OPP) was also less than expected at 32.1 mmHg. See the FAT1 Ophthalmodynamometry Result Screen.
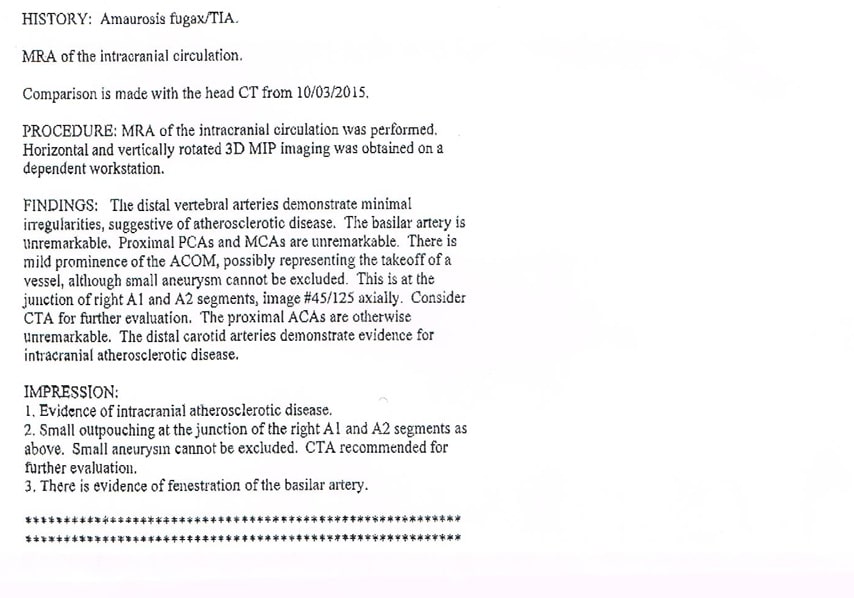
Because the history and the FAT1 results were suggestive of carotid vascular disease, an intracranial Magnetic Resonance Imaging Arteriogram was performed which confirmed atherosclerotic carotid vascular disease and raised the possibility of an anterior communicating artery aneurysm. See the MRA report. A CTA was scheduled for further evaluation.
The CTA confirmed an anterior communicating artery aneurysm.
Pigmentary Glaucoma
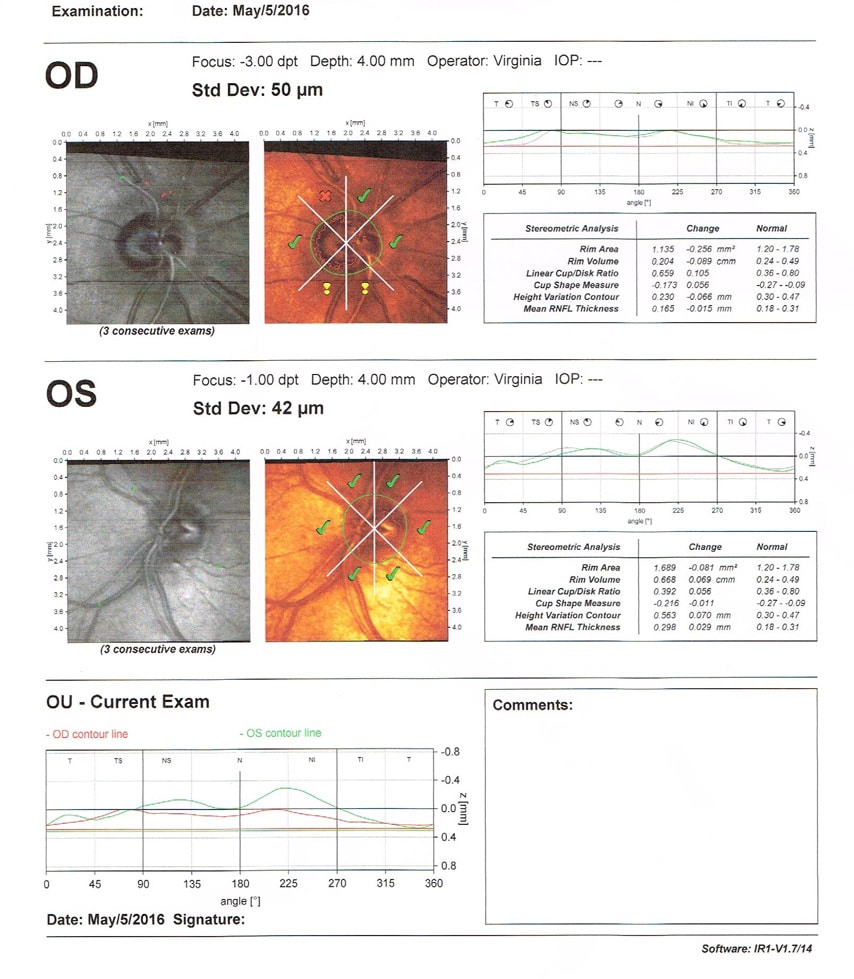
An 57 year old male with Pigmentary Glaucoma in the right eye presented with elevated Intraocular Pressure (IOP). Current medications were Combigan BID, Pilocarpine 1% TID, Travatan QHS and Diamox 500 mg BID. On gonioscopy the angle was open with 4+ pigment. Laser Trabeculoplasty was performed. The IOP remained elevated at 30 mmHg well above the target value. Heidelberg Retinal Tomography documented progressive thinning of the nerve fiber layer at 6 and 12 o’clock. See the HRT results.
The Tonography Function of the FAT1 Device was used to assess Trabecular Meshwork Aqueous Humor Outflow. Aqueous Humor Outflow was reduced at 0.109 microliters / minute and the ratio of the IOP (Po) to Outflow (C), Po / C Ratio, was 204.6. See FAT1 Tonography Results Screen.
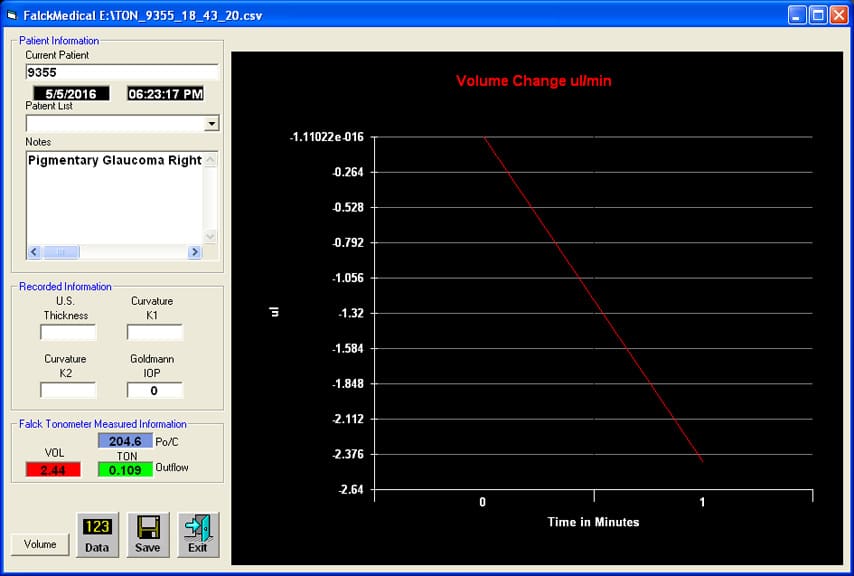
In the FAT1 Tonography Clinical Study, Glaucomatous eyes had an Outflow Value less than 0.18 microliters / minute. A Po / C ratio greater than 100 is characteristic of glaucomatous eyes (Chandler and Grants Glaucoma, Fourth Edition, Chapter 6, Tonometry and Tonography, page 45 – 48).
Visual field testing was performed. The decreased outflow facility, which did not respond to medical or laser surgery, was the cause of the elevated IOP. The patient underwent a trabeculectomy to bypass the dysfunctional trabecular meshwork.
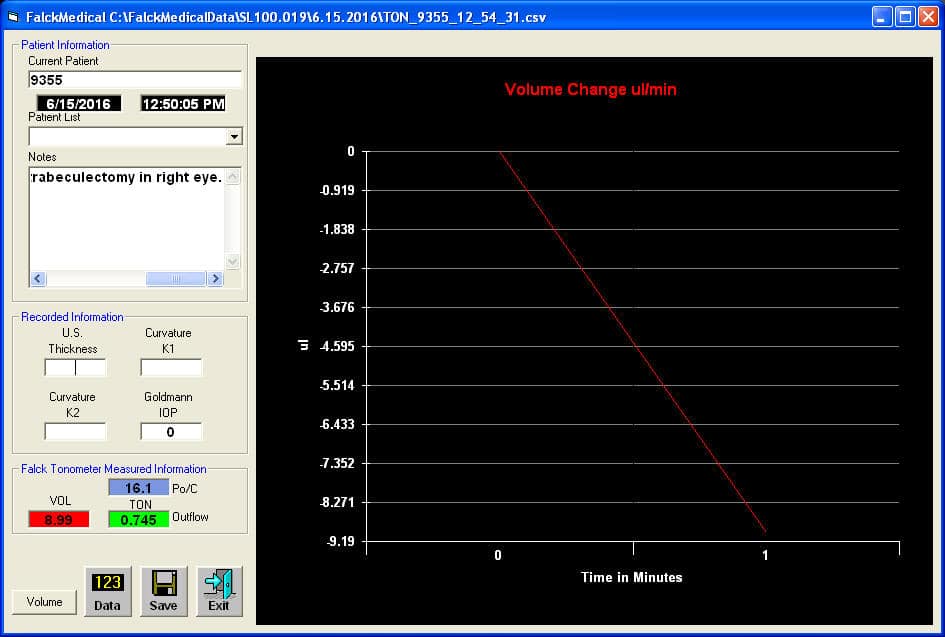
The Tonography function of the FAT1 device was used to assess aqueous humor outflow after the trabeculectomy procedure. Outflow was increased to 0.745 microliters / minute, confirming the effectiveness of the trabeculectomy. See the post-trabeculectomy procedure FAT1 Tonography Results Screen.
Angle Closure / Pupillary Block
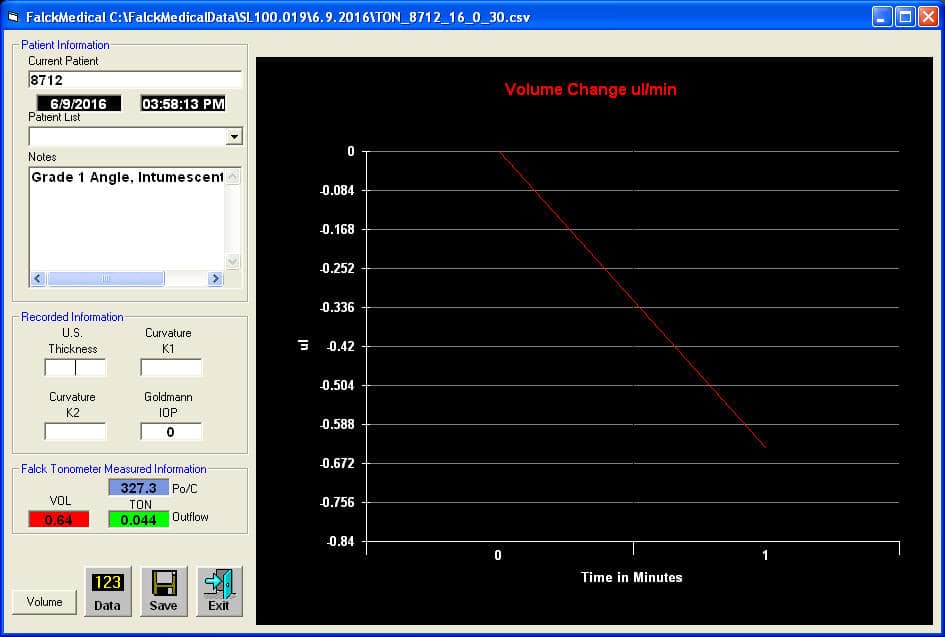
A 67 year old male presented with an intumescent count fingers cataract in the right eye. Pupillary block was present. On direct gonioscopic examination the anterior chamber angle was closed at Grade 1. In the left eye and the anterior chamber angle was open at Grade 4.
The Tonography function of the FAT1 device was used to assess aqueous humor outflow through the trabecular meshwork. It was reduced to 0.044 microliters / minute and the Po / C ratio was increased at 327.3. See the FAT1 Tonography Results Screen for the Right Eye.
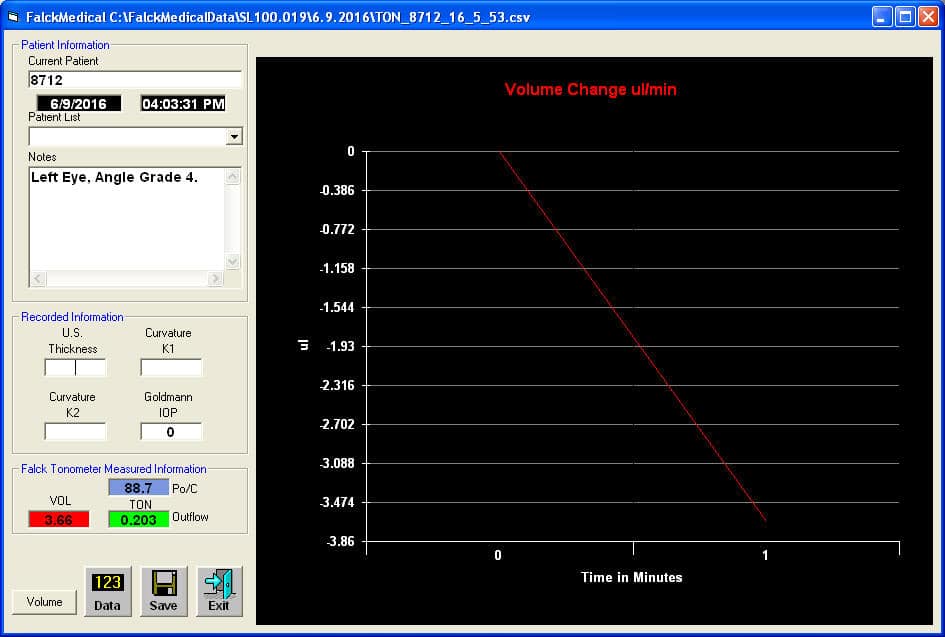
In the left eye, the aqueous humor outflow was 0.203 microliters / minute and the Po / C ratio was 88.7. See the FAT1 Tonography Results Screen for the left eye.
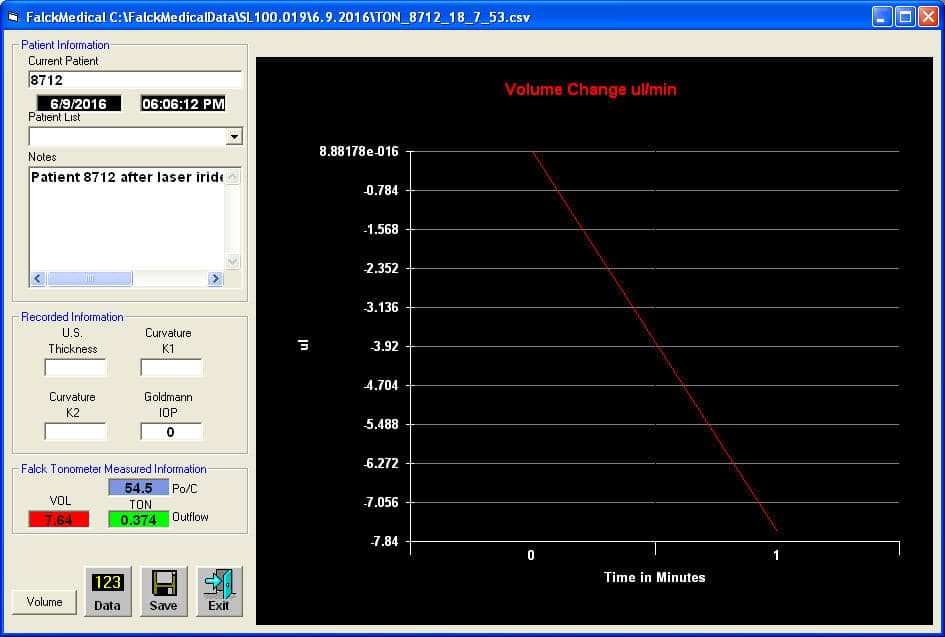
One percent Pilocarpine was placed in the right eye and a YAG Laser Peripheral Iridectomy was performed. The pupillary block decreased and the anterior chamber angle deepened to Grade 3.
Aqueous humor outflow was assessed post-iridectomy using the Tonography Function of the FAT1 Device. It increased to 0.374 microliters / minute, confirming the effectiveness of the iridectomy. See the post-iridectomy FAT1 Tonography Results Screen.